
Shock Blocks: A Better Way to Understand Shock Without Making Your Brain Tap Out
Shock is one of those EMS topics that seems simple right up until it is not.
On paper, shock is poor perfusion. Easy enough. The body is not moving enough oxygen, glucose, and nutrients to the cells. Waste products are building up. Organs are getting cranky. The brain starts acting differently. The heart is working harder. Breathing changes. Blood pressure may drop. Everyone starts having a bad day.
On paper, shock is poor perfusion. Easy enough. The body is not moving enough oxygen, glucose, and nutrients to the cells. Waste products are building up. Organs are getting cranky. The brain starts acting differently. The heart is working harder. Breathing changes. Blood pressure may drop. Everyone starts having a bad day.
What Are Shock Blocks?
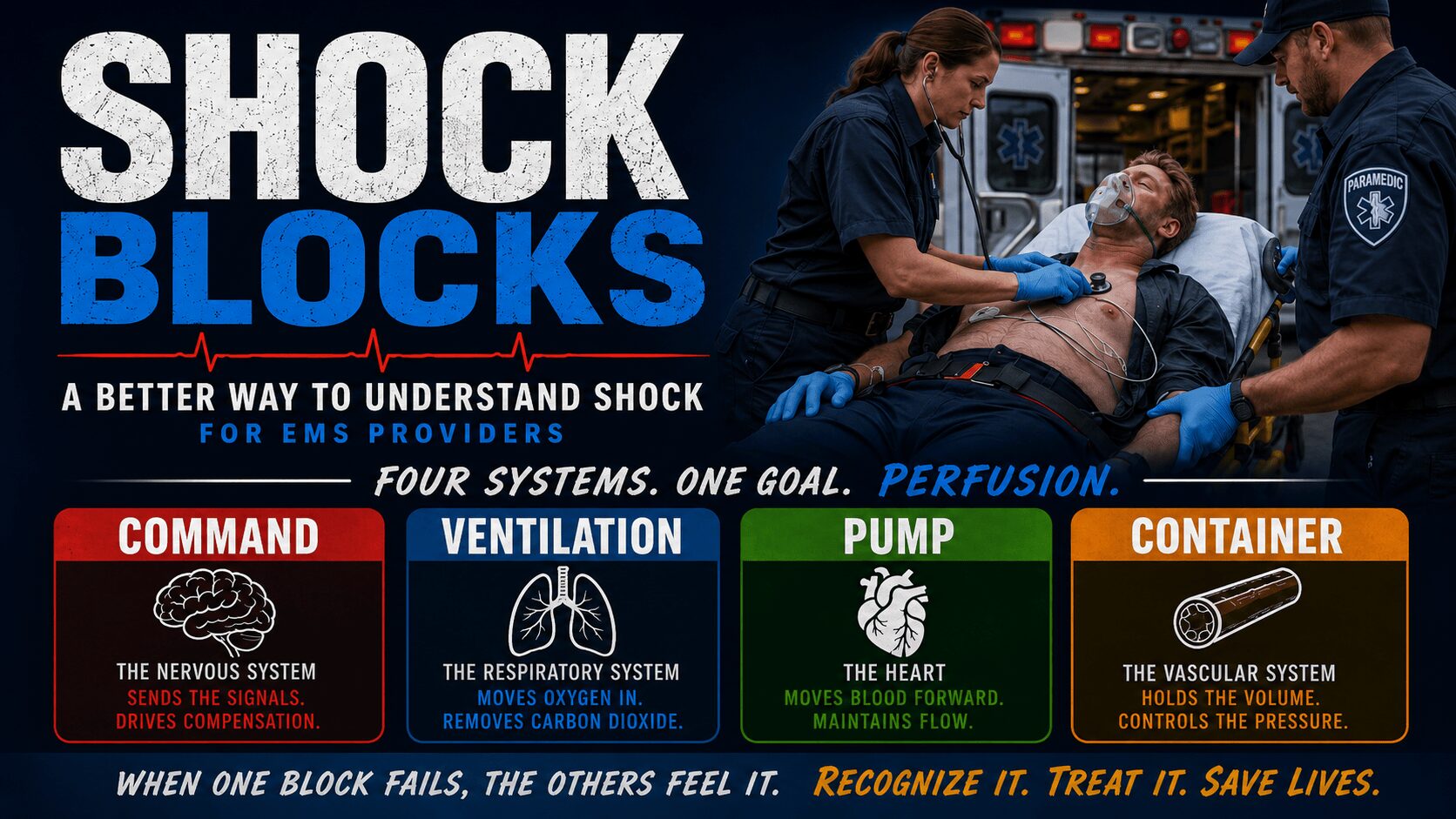
Shock Blocks is a simple way to understand shock by breaking the body’s perfusion system into four major parts:
- Command
- Ventilation
- Pump
- Container
On paper, shock is poor perfusion. Easy enough. The body is not moving enough oxygen, glucose, and nutrients to the cells. Waste products are building up. Organs are getting cranky. The brain starts acting differently. The heart is working harder. Breathing changes. Blood pressure may drop. Everyone starts having a bad day.
Why I Made the Shock Blocks Video Series
I created the Shock Blocks video series to make shock easier to understand for EMRs, EMTs, PCPs, ACPs, paramedic students, and practicing EMS providers.
Shock is often taught by listing types and memorizing signs and symptoms. That can work for a test, but it does not always help on scene. In the field, you need to recognize what is happening, why it is happening, and what problem you are trying to fix.
The Shock Blocks system gives you a mental model.
Instead of asking, “What shock type is this?” as your first question, you can ask:
Which block is failing?
That question helps organize your thinking.
Is the heart unable to pump? That points toward a Pump problem.
Is the patient losing blood or fluid? That points toward a Container problem.
Is the vascular system wide open and unable to constrict? That is also a Container problem, but for a different reason.
Is the nervous system unable to send the right signals? That brings in the Command block.
Is oxygen not getting in or carbon dioxide not getting out? That brings in the Ventilation block.
This does not replace clinical judgment. It supports it.
Think of Shock Blocks as a way to stop your brain from opening 47 tabs at once during a sick patient call.
The Stages of Shock
The first video in the series introduces the stages of shock.
Watch it here:
Shock does not usually go from “fine” to “cardiac arrest” in one neat step. It progresses.
The early stages may be subtle. The patient may still have a blood pressure that looks acceptable. They may still answer questions. They may still be walking around, which is always inconvenient when their physiology is quietly waving a red flag.
A useful way to think about shock progression is:
- Normal or asymptomatic
- Behaviour change
- Compensated shock
- Decompensated shock
- Irreversible shock
- Cardiac arrest
The behaviour change stage matters. Restlessness, anxiety, confusion, or the patient saying they feel wrong may be an early sign that perfusion is starting to fail.
In compensated shock, the body is working hard to maintain perfusion. Heart rate may increase. Respiratory rate may increase. The vascular system may constrict. The body is trying to keep blood moving to the brain, heart, and vital organs.
In decompensated shock, those compensatory systems begin to fail. Blood pressure may drop. Level of consciousness may worsen. Skin signs may change. The patient may no longer be able to maintain adequate perfusion.
By irreversible shock, the body has sustained severe cellular and organ damage. At that point, treatment becomes much harder.
That is why waiting for the blood pressure to crash before taking shock seriously is not a great strategy. It is a bit like waiting until the kitchen is on fire before wondering if the smoke alarm was trying to tell you something.
Cardiogenic Shock: When the Pump Fails
Watch the cardiogenic shock video here:
Cardiogenic shock is a Pump block problem.
The heart itself is not able to pump blood effectively. That can happen for several reasons.
The patient may have a rhythm problem. If the heart rate is too slow, the heart may not move enough blood forward. If the heart rate is too fast, the ventricles may not have enough time to fill. Either way, cardiac output can drop.
The patient may have poor contractility. The heart muscle may not squeeze strongly enough to push blood forward.
The patient may be having a myocardial infarction. If part of the heart muscle is not getting enough oxygen, that section may not work properly. The pump becomes weaker.
The patient may also have physical damage to the heart, such as from trauma.
In cardiogenic shock, the key issue is that the heart is failing as a pump. When the pump fails, oxygen delivery drops. Carbon dioxide removal may suffer. Glucose and nutrients do not reach cells effectively. The Command, Ventilation, and Container blocks all start reacting to the Pump problem.
EMS care depends on scope and protocol, but one universal point is this:
Do not make the heart work harder than it already is.
Minimize exertion. Do not make the patient walk when they should be moved. Support oxygenation and ventilation as needed. Follow local protocols for medications and advanced care.
A failing heart does not need a fitness challenge.
Obstructive Shock: When Something Stops the Pump
Watch the Obstructive Shock video here.
Obstructive shock can look similar to cardiogenic shock because the Pump block is affected. The difference is that the heart itself may not be the original problem.
In obstructive shock, something outside the heart prevents it from filling, pumping, or moving blood forward properly.
Common causes include:
- Tension pneumothorax
- Pulmonary embolism
- Cardiac tamponade
- Major vessel obstruction
A tension pneumothorax can create pressure inside the chest. As that pressure builds, it can shift structures, compress the heart, and interfere with venous return. Less blood returns to the heart. Less blood fills the heart. Less blood gets pumped out.
That means decreased preload and decreased cardiac output.
Cardiac tamponade works differently but creates a similar problem. Fluid builds up in the pericardial sac around the heart. The heart becomes restricted and cannot fill or squeeze properly.
A pulmonary embolism can block blood flow through the pulmonary circulation. Blood cannot move through the lungs properly, which affects oxygenation and cardiac output.
The heart may be trying. The heart may even be capable. But something is physically getting in the way.
Very rude.
In Shock Blocks language, obstructive shock affects the Pump block because the pump cannot function normally, but the cause is external obstruction.
Hypovolemic Shock: When the Container Is Empty
Watch the Hypovolemic Shock video here.
Hypovolemic shock is mainly a Container block problem.
The body does not have enough circulating volume inside the vascular system. That volume may be lost through bleeding, dehydration, vomiting, diarrhea, sweating, poor intake, or trauma.
In trauma, the obvious version is external bleeding. Blood is leaving the body and collecting somewhere it does not belong, such as the ground. The ground does not need perfusion. The brain does.
Major external bleeding needs early control. Direct pressure, tourniquets, wound packing, and other bleeding control methods depend on the injury and scope of practice.
Internal bleeding is trickier because you may not see it. A patient can lose a significant amount of blood into the abdomen, pelvis, chest, or soft tissues before it becomes obvious. Mechanism of injury matters. So do vital signs, skin signs, level of consciousness, and patient presentation.
Hypovolemic shock can also come from dehydration. A patient with severe vomiting and diarrhea can lose enough fluid to compromise perfusion. A person exercising in heat can sweat out enough fluid to become seriously volume depleted.
In Shock Blocks terms, the Container block is losing volume. The body may try to compensate by constricting the vascular system, increasing heart rate, and increasing respiratory rate. That may work for a while.
But if the container keeps emptying, compensation has limits.
The heart cannot pump what it does not have.
That is not motivational. It is physiology.
Distributive Shock: When the Container Cannot Constrict
Watch the Distributive Shock video here.
Distributive shock is also a Container block problem, but it is different from hypovolemic shock.
In hypovolemic shock, the container may be the right size, but there is not enough volume.
In distributive shock, the patient may have volume, but the container becomes too large or too relaxed to maintain pressure.
The vascular system loses its ability to constrict effectively. Blood is not distributed properly. Pressure drops. Perfusion fails.
The three major subtypes covered in the series are:
- Septic shock
- Anaphylactic shock
- Neurogenic shock
Each one has different causes and treatment priorities, but they share a common theme: vascular tone is not working properly.
The container opens up, and the body struggles to maintain perfusion.
Septic Shock: When Infection Becomes a Perfusion Problem
Watch the Spetic Shock video here.
Septic shock is a form of distributive shock caused by severe infection and the body’s response to that infection.
Common sources may include:
- Pneumonia
- Urinary tract infection
- Cellulitis
- Other serious infections
These patients may have been sick for more than a day. They may have fever, chills, sweating, weakness, altered mental status, or low blood pressure. Some may be hypothermic instead of febrile, especially when they are very sick.
Sepsis can cause widespread inflammation, vasodilation, capillary leak, and poor vascular control. Fluid can leave the vascular space and move into tissues. The vascular system may not constrict properly. Blood pressure may fall.
The heart and lungs often try to compensate. Heart rate increases. Respiratory rate increases. The patient may look very unwell because they are, in fact, very unwell.
EMS care may include supportive care, oxygen as needed, ventilation support if required, fluids within scope and protocol, vasopressors for advanced providers when indicated, early transport, and hospital notification.
Hospital notification matters because septic patients often need antibiotics, fluids, vasopressors, lab work, and ongoing resuscitation. EMS cannot fix the infection in the living room, which is annoying but true.
We can recognize the problem, support perfusion, and get the patient to definitive care.
Anaphylactic Shock: When the Immune System Overreacts
Watch the Anaphylactic Shock video here.
Anaphylaxis is another form of distributive shock.
An allergic reaction may affect one body system, such as hives on the skin. Anaphylaxis is more serious because it involves more than one body system or includes airway, breathing, or circulation concerns.
The patient may have:
- Hives
- Swelling
- Shortness of breath
- Wheezing
- Nausea
- Vomiting
- Tongue or lip swelling
- Airway involvement
- Hypotension
Anaphylaxis involves a major immune response with histamine release. Histamine causes vasodilation and increased capillary permeability. In plain language, the vessels open up and fluid leaks into places where it becomes a problem.
The airway can swell. The tongue can swell. The lungs can become wheezy. Blood pressure can drop. Perfusion can fail quickly.
This is why epinephrine matters.
Epinephrine is the first-line treatment for anaphylaxis, within scope and protocol. It helps with vasoconstriction, bronchodilation, and supporting blood pressure. It can push several blocks back toward where they belong.
Benadryl is not the first priority in true anaphylaxis. It may have a role depending on protocol, but it does not replace epinephrine.
If the patient improves after epinephrine, that does not mean the call is over. Symptoms can return. These patients still need assessment, monitoring, and transport according to local protocols.
Anaphylaxis can look dramatic because it is dramatic. The good news is that early epinephrine can make a major difference.
Neurogenic Shock: When the Signal Is Broken
Watch the Neurogenic Shock video here.
Neurogenic shock is also a type of distributive shock, but it has a very different presentation.
It usually results from damage to the spinal cord or central nervous system. The body loses sympathetic tone. The normal fight-or-flight signals are disrupted.
That sympathetic response normally helps increase heart rate, increase respiratory drive, and constrict the vascular system.
In neurogenic shock, that signal may not get through.
The result can be:
- Hypotension
- Bradycardia
- Warm, flushed, dry skin
- Poor vascular tone
- Limited compensation
This is different from many other shock presentations. In many shock states, the patient becomes pale, cool, sweaty, and tachycardic as the body attempts to compensate. In neurogenic shock, the patient may be hypotensive and bradycardic because the body cannot mount the same response.
In Shock Blocks terms, neurogenic shock affects the Command block and the Container block.
The Command block cannot send the right signal. The Container block cannot constrict properly. The vascular system opens up. Blood pressure drops. The heart rate may not increase the way you expect.
These patients need supportive care, spinal precautions as indicated, oxygenation and ventilation support when required, early transport, and ALS support when needed.
The key is recognizing that this shock state does not always look like the others.
Warm, dry, bradycardic, and hypotensive after a spinal cord injury should get your attention.
Why Early Recognition Matters
Shock is easier to treat early.
That sentence should be printed on a sticker and placed somewhere EMS providers will see it before every call.
Once the patient is decompensating, multiple systems may be failing. The heart may be struggling. The lungs may be struggling. The brain may be underperfused. The vascular system may be unable to maintain pressure. The patient may be acidotic, hypoxic, hypotensive, or altered.
At that point, treatment is harder.
Early shock may be subtle. It may be a behaviour change. Anxiety. Restlessness. Mild confusion. A feeling that something is wrong. A high-risk mechanism. A sick-looking infection patient. A trauma patient with hidden bleeding. A chest pain patient who looks worse than the monitor suggests.
The goal is not to memorize every possible sign and symptom in isolation.
The goal is to recognize patterns.
Ask yourself:
- Is the Pump working?
- Is the Container full?
- Can the Container constrict?
- Is Ventilation adequate?
- Is Command sending the right signals?
- Is the patient compensating?
- Is compensation starting to fail?
That framework can help organize your assessment and treatment priorities.
Take the Full Shock Blocks Course
The full course includes more lessons, case examples, quizzes, downloadable resources, and a certificate that can be submitted to the Alberta College of Paramedics for continuing education credit.
Take the full Shock Blocks course here:
If you are an EMR, EMT, PCP, ACP, paramedic student, or practicing EMS provider, this course is built to help you understand shock in a way that works on real calls, not just in textbook chapters.
Shock is complex, but it does not have to feel like a mystery wrapped in a blood pressure cuff.
Break it into blocks.
Find the failing system.
Treat the right systems with the right treatment.
Recognize deterioration early.
And please, do not wait for the blood pressure to crash before you believe the patient is sick.